This study was conducted in an experimental setting where fentanyl was infused over an extended period and titrated to maintain consistent plasma concentrations. As such, the clinical implications of these findings for real-world overdose situations are unknown.
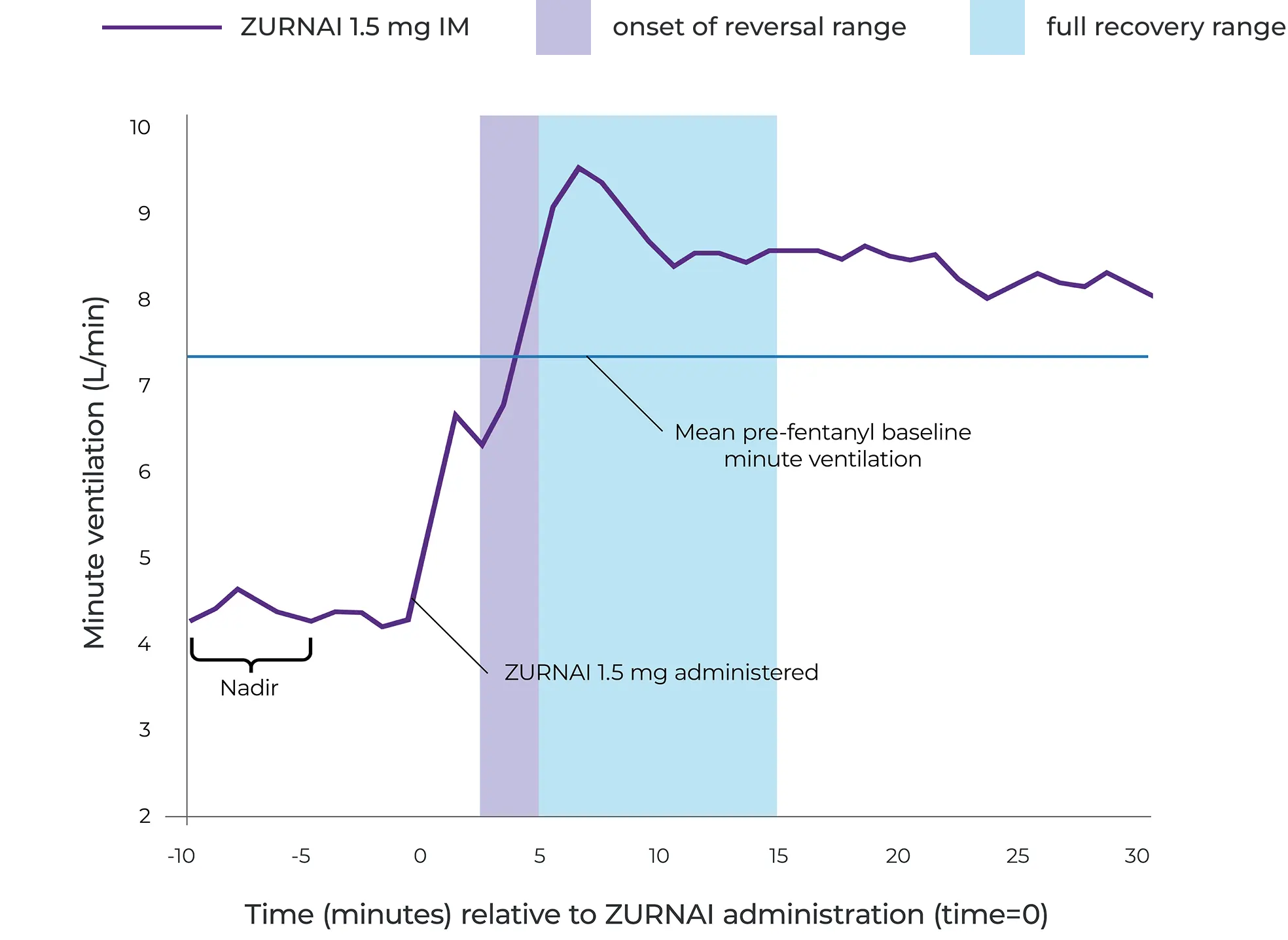
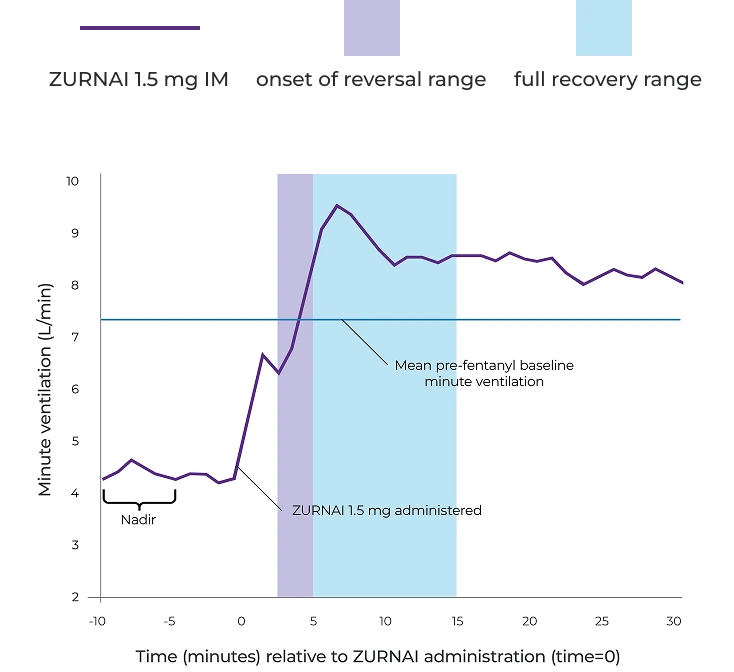
Following ZURNAI administration, the time to onset of reversal of respiratory depression was observed between 2.5 to 5 minutes
At 5 minutes, mean change in minute ventilation (MV) from nadir* was 4.42 L/min
Full recovery of respiratory drive was noted between 5 and 15 minutes after ZURNAI administration
*MV nadir was defined as a 50% reduction in MV from baseline or the MV reduction achieved following the maximum permitted fentanyl titration.
Pharmacodynamic study assessed the ability of ZURNAI to reverse respiratory depression1
An experimental clinical opioid-induced respiratory depression (OIRD) model assessed pharmacodynamic effects of ZURNAI, specifically changes in minute ventilation (MV) during administration of a 3-step intravenous fentanyl infusion.
Participants: 24 healthy adult subjects who were opioid-experienced and non-opioid dependent.
NAL1004 study design
STEP 1
Fentanyl was infused until MV nadir* (functional OIRD) was achieved
STEP 2
Following attainment of MV nadir, fentanyl infusion rate was decreased to maintain the fentanyl concentrations
ZURNAI was administered at 10 minutes following MV nadir
STEP 3
10 minutes following ZURNAI administration, fentanyl infusion rate was further decreased to maintain constant fentanyl concentrations for remaining duration of reversal session
*MV nadir was defined as a 50% reduction in MV from baseline or the MV reduction achieved following the maximum permitted fentanyl titration.
*MV nadir was defined as a 50% reduction in MV from baseline or the MV reduction achieved following the maximum permitted fentanyl titration.
This study was conducted in an experimental setting where fentanyl was infused over an extended period and titrated to maintain consistent plasma concentrations. As such, the clinical implications of these findings for real-world overdose situations are unknown.1
Reversal of fentanyl-induced respiratory depression in adult healthy volunteers treated with ZURNAI1
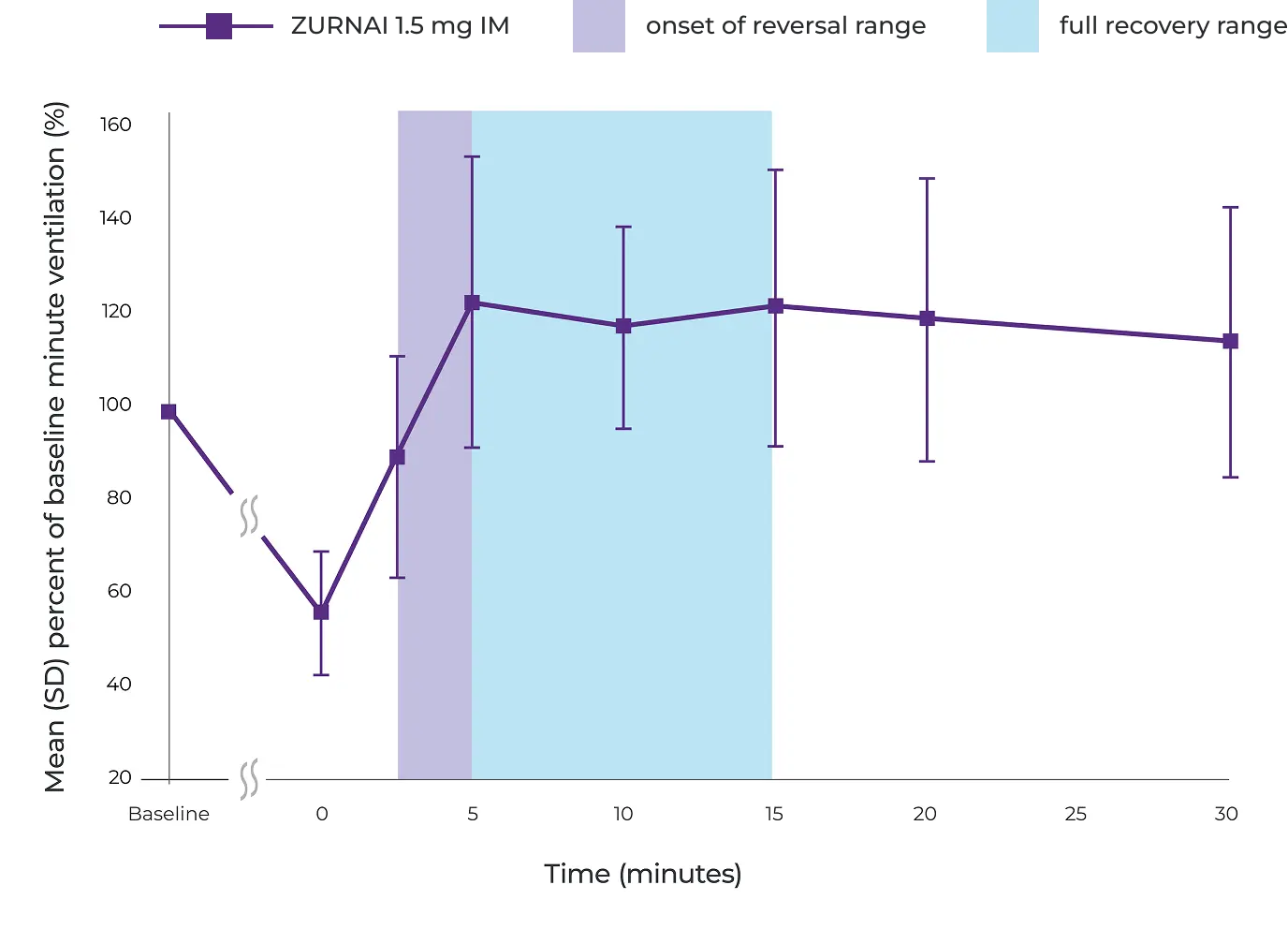
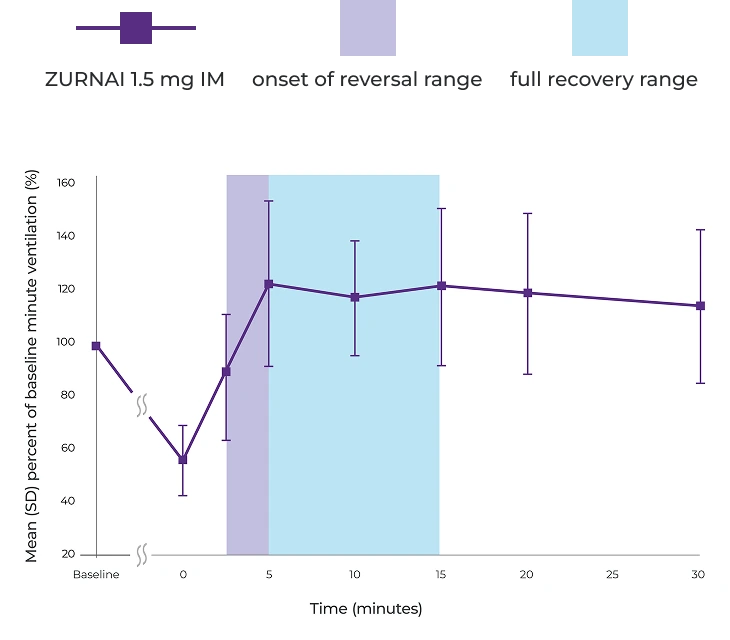
Percent recovery of respiratory drive after fentanyl infusion in minute ventilation (mean SD) in adult healthy volunteers with ZURNAI 1.5 mg1
IM=intramuscular; SD=standard deviation.
Actor portrayals.
Pharmacokinetic study key findings1†
ZURNAI has a long half-life1‡
Pharmacokinetic (PK) Study NAL10051
To determine the relative bioavailability of ZURNAI, one dose was administered intramuscularly (IM) in 24 healthy adult subjects. A 1.0 mg dose of nalmefene administered as an IM injection was used as a comparator.
While the duration of action of nalmefene is as long as most opioids,§ a recurrence of respiratory depression is possible, even after an apparently adequate initial response to ZURNAI treatment.
Therefore, it is necessary to seek emergency medical assistance immediately after administration of the first dose of ZURNAI and to keep the patient under continued surveillance. A second dose may be necessary if there is recurrence of symptoms of opioid overdose.
†Pharmacokinetic studies are conducted in healthy subjects; as such, the clinical implications of these findings for real-world overdose situations are unknown.
‡ZURNAI mean elimination half-life of 9.07 hours is based on a pharmacokinetic study of 24 healthy adult subjects given a single dose of intramuscular ZURNAI.1
§The half-life of fentanyl used as anesthesia has been shown to be about 7.5 hours; the half-life of illicit fentanyl has not been characterized.2
In the PK study NAL1005, the mean TERMINAL elimination half-life of ZURNAI was 9.07 hours1
Pharmacokinetic studies are conducted in healthy subjects; as such, the clinical implications of these findings for real-world overdose situations are unknown.
Key pharmacokinetic parameters in healthy volunteers (n=24)
Drug
ZURNAI IM 1.5 mg
Cmax (ng/mL)‖
7.37 (47.5)
Tmax (hours)¶
0.25 (0.083-1.00)
Half-life (hours)#
9.07 (26.6)
Nalmefene IM 1.0 mg
Cmax(ng/mL)‖
2.39 (32.6)
Tmax (hours)¶
0.50 (0.083-2.00)
Half-life (hours)#
7.74 (24.3)
Nalmefene IV 1.0 mg
Cmax (ng/mL)‖
6.94 (55.7)
Tmax (hours)¶
0.083 (0.083-0.250)
Half-life (hours)#
9.12 (16.5)
Drug
Cmax (ng/mL)‖
Tmax (hours)¶
Half-life (hours)#
ZURNAI IM 1.5 mg
7.37 (47.5)
0.25 (0.083-1.00)
9.07 (26.6)
Nalmefene IM 1.0 mg
2.39 (32.6)
0.50 (0.083-2.00)
7.74 (24.3)
Nalmefene IV 1.0 mg
6.94 (55.7)
0.083 (0.083-0.250)
9.12 (16.5)
Cmax=maximum concentration; IV=intravenous; Tmax=time to maximum concentration.
‖Presented as geometric mean (coefficient of variation percentage).
¶Presented as median (range).
#Presented as arithmetic mean (coefficient of variation percentage).
Not actual size.
Clinically demonstrated safety profile1
The safety of ZURNAI is supported by a pharmacokinetic study of healthy adults under normal conditions and by a pharmacodynamic study evaluating the effects of ZURNAI under steady-state opioid infusion.1
ZURNAI: Important considerations
ZURNAI is not a substitute for emergency care1
Use ZURNAI with extreme caution in patients with known physical dependence on opioids, as acute withdrawal symptoms may occur1
Any attempt to overcome receptor blockade from opioid antagonists such as ZURNAI with large doses of opioids may lead to opioid intoxication and death1
Reversal of respiratory depression caused by partial agonists or mixed agonist/antagonists, such as buprenorphine and pentazocine, may be incomplete and may require repeated administration of ZURNAI using a new auto-injector1
Relative frequencies of most common adverse reactions that occurred in greater than 5% of subjects in Study NAL1004 and Study NAL10051
System organ class Adverse event
Pooled NAL1004 and NAL1005 N=44 n (%)
Any adverse reaction
28 (63.6)
Nervous system disorders
Dizziness
7 (15.9)
Headache
8 (18.2)
Allodynia
5 (11.4)
Burning sensation
3 (6.8)
Gastrointestinal disorders
Nausea
8 (18.2)
Vomiting
5 (11.4)
Ear and labyrinth disorders
Tinnitus
4 (9.1)
Ear discomfort
3 (6.8)
System organ class Adverse event
Pooled NAL1004 and NAL1005 N=44 n (%)
Cardiac disorders
Palpitations
4 (9.1)
General disorders and administration-site conditions
Feeling hot
11 (25.0)
Chills
6 (13.6)
Feeling abnormal
3 (6.8)
Vascular disorders
Hot flush
3 (6.8)
Psychiatric disorders
Irritability
3 (6.8)
It is necessary to seek emergency medical assistance immediately after administration of the first dose of ZURNAI and to keep the patient under continued surveillance.1
ZURNAI is indicated for the emergency treatment of known or suspected opioid overdose induced by natural or synthetic opioids in adults and pediatric patients aged 12 years and older, as manifested by respiratory and/or central nervous system depression.
ZURNAI is intended for immediate administration as emergency therapy in settings where opioids may be present.
ZURNAI is not a substitute for emergency medical care.
Important Safety Information and Indications and Usage
CONTRAINDICATIONS
ZURNAI is contraindicated in patients known to be hypersensitive to nalmefene hydrochloride or to any other ingredients in the product.
WARNINGS AND PRECAUTIONS
Risk of Recurrent Respiratory and Central Nervous System Depression
A recurrence of respiratory depression is possible, therefore, keep the patient under continued surveillance and administer repeat doses of ZURNAI if necessary, using a new auto-injector with each dose while awaiting emergency medical assistance.
Risk of Limited Efficacy with Partial Agonists or Mixed Agonist/Antagonists
Reversal of respiratory depression by partial agonists or mixed agonists/antagonists such as buprenorphine and pentazocine, may be incomplete. Repeat doses of ZURNAI may be required.
Precipitation of Severe Opioid Withdrawal
The use of ZURNAI in patients who are opioid dependent may precipitate opioid withdrawal.
Abrupt postoperative reversal of opioid depression may result in adverse cardiovascular (CV) effects. These events have primarily occurred in patients who had preexisting CV disorders or received other drugs that may have similar adverse CV effects. Monitor these patients closely in an appropriate healthcare setting after use of ZURNAI.
In neonates, opioid withdrawal may be life-threatening if not recognized and properly treated and may include the following signs and symptoms: convulsions, excessive crying, and hyperactive reflexes. Monitor the patient for the development of the signs and symptoms of opioid withdrawal.
Risk of Opioid Overdose from Attempts to Overcome the Blockade
Attempts to overcome opioid withdrawal symptoms caused by opioid antagonists with high or repeated doses of exogenous opioids may lead to opioid intoxication and death.
ADVERSE REACTIONS
Most common adverse reactions (> 5%) are feeling hot, nausea, headache, dizziness, chills, vomiting, allodynia, palpitations, tinnitus, ear discomfort, feeling abnormal, burning sensation, hot flush, and irritability.
USE IN SPECIFIC POPULATIONS
Pregnancy
An opioid overdose is a medical emergency and can be fatal for the pregnant woman and fetus if left untreated. Treatment with ZURNAI for opioid overdose should not be withheld because of potential concerns regarding the effects of ZURNAI in the fetus.
Pediatric Use
The safety and effectiveness of ZURNAI for the emergency treatment of known or suspected opioid overdose, as manifested by respiratory and/or central nervous system depression, have not been established in pediatric patients younger than 12 years of age.
Geriatric Use
Clinical studies of nalmefene hydrochloride injection did not include sufficient number of subjects aged 65 and over to determine whether they respond differently from younger subjects.
Please read
To report SUSPECTED ADVERSE REACTIONS, contact Knoa Pharma LLC at 1 888-726-7535, option 2, or FDA at 1-800-FDA-1088 or .
Intended for healthcare professionals of the United States of America only.
2. Ahonen J, Olkkola KT, Hynynen M, et al. Comparison of alfentanil, fentanyl and sufentanil for total intravenous anaesthesia with propofol in patients undergoing coronary artery bypass surgery. Br J Anaesth. 2000;85(4):533-540. doi:10.1093/bja/85.4.533.